If you are an engineer, your plan—bottom line, no fudging about—has to WORK. All. The. Time. It’s what we expect from engineers.
On the other hand, if you are a Government-Approved Nutrition Expert, your plan doesn’t have to work AT ALL.
Which may be why we don’t let Nutrition Experts build bridges.
To ensure a more impressive rate of success, engineers tend to build their bridges and elevators based on a few mysterious but fundamental concepts like physics (or as we say around here, fweezix). Now, to paraphrase Barbie, I understand that physics is TOUGH. But it is also, well, insurmountably the real deal, and anything that defies the laws of physics is generally—for lack of a better word—considered to be magic.
Now, from my biochemistry classes, it looks like the principles of nutrition are built on chemistry, and the principles of chemistry are built on—you guessed it!—politics physics But when I step across the hall to my public health classes, then the principles of nutrition are based on the Dietary Guidelines, which—as they tend to be in defiance of the laws of physics—I guess must be magic!
Despite the rockin’ groove, I’m not sure that I believe in magic.
But Calories In = Calories out is not magic, it’s physics, right? It seems indisputable—a veritable law of thermodynamics—that if you consume fewer calories than you expend, you will lose weight. Conversely, if you consume more calories than you expend, you will gain weight. Duh.
Sometimes when things aren’t working (i.e. major bridge oopie ), we get a glimpse of the realities of the physics behind the system. Let’s take a look at a category of individuals that do lose weight easily—too easily: Type 1 diabetics. A type 1 diabetic could eat 5000 calories a day, never move a muscle, and still lose weight (for the record: this is not a good thing). What happens to those calories? Why don’t they get stored as fat (hello? calories IN?) A type 1 diabetic can’t store them as fat. Why not? No insulin. Without insulin, the body cannot store energy at all. Type I diabetics must be given insulin or they literally waste away. It’s not because they try harder; it’s because of physics.
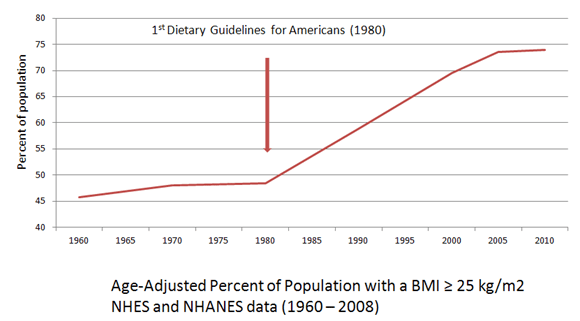
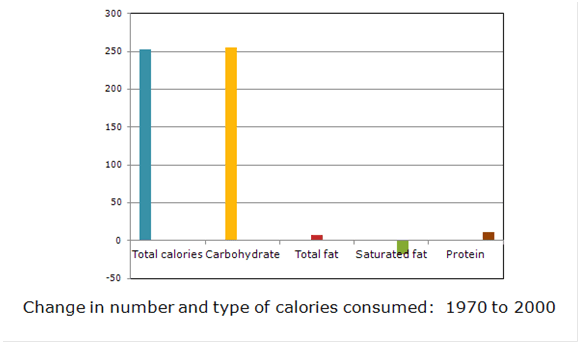
What this means is that it can’t just be the amount of calories that we are consuming, but also the source. And in the case of unnecessary carbohydrates in the diet, it’s likely to be both. The increase in caloric intake we’ve seen in the past 30 years has come almost entirely from industrialized carbohydrate food products—subsidized and endorsed by the USDA.
Would obesity rates have skyrocketed without the Guidelines prompting Americans to eat fewer animal products—especially meat and eggs which contain Very Scary saturated fat and cholesterol—and more whole grain cereal products? We’ll never know. But physics does tell us that carbohydrate foods have particular qualities that affect fat storage and metabolism, specifically: “A high carbohydrate meal stimulates the production of insulin. Insulin inhibits the body’s ability to use fat for energy and stimulates the uptake of fat and its storage as triacylglycerol” (Campbell & Farrell, 2009). That’s straight from my biochemistry textbook.
Now I don’t care if you eat carbs or not. Some of my best friends are carbs. But can we stop pretending that somehow—magically—there’s no relationship between the two figures above?
Apparently we can’t. According to many Nutrition Experts, including Marion Nestle, our low-fat Dietary Guidelines can be blamed only in that they do not do more to “address caloric intake, portion size, inactivity, and other contributors to obesity” (Woolf & Nestle, 2008). Notice that “caloric intake,” “portion size” and “inactivity” are all things that are our fault—in contrast to a diet recommendation of mostly carbohydrates, something the USDA and HHS are responsible for. In other words, if chubby little Americans can’t “achieve energy balance” by eating less and exercising more, it’s not because the Guidelines aren’t helping us, it’s because we are simply not trying hard enough.
(True Confession: I mostly just wanted to draw that cartoon.)
Should we reduce our calories? Maybe not a bad idea for some folks.
What kind of calories should we reduce? Ask an engineer. Unless you believe in magic . . .
References:
Campbell MK, Farrell SO. Biochemistry, 6th ed. United States: Thomson, 2009. p. 730.
Centers for Disease Control and Prevention (CDC). Trends in intake of energy and macronutrients–United States, 1971-2000. Morbidity and Mortality Weekly Report. 2004 Feb 6;53(4):80-2.
Woolf SH, Nestle M. Do dietary guidelines explain the obesity epidemic? American Journal of Preventive Medicine. 2008 Mar;34(3):263-5.

I agree that it is more complicated than “calories-in, calories-out” but I’m hesitant with your specific example of why this isn’t so. A type one diabetic won’t gain weight after eating 5000 calories ONLY if they aren’t taking insulin. The person in this example wouldn’t be around long to enjoy that lifestyle as type 1 diabetics cannot live long without outside insulin before going into diabetic ketoacidosis. This seems to be more of an exception to the rule of “calories-in, calories-out” than a disproval. Along the similar lines would be someone malabsorping fat. Thoughts? Thanks for your site.
The difference with the malabsorption of fat is that for Type 1 diabetes, the glucose *is* absorbed. But the body does not respond to this absorption in a typical fashion. With fat malabsorption, the fat never makes it from “outside” the body (which the GI tract sort of still is) to “inside.” Before advent of insulin, people with Type 1 diabetes were treated with very low carbohydrate and very high fat diets. Insulin is not necessary (although it does enhance) the uptake of amino acids necessary for growth, and there is a constant amount of non-insulin mediated glucose uptake occurring in the body. Of course, I would never argue that insulin shouldn’t be used for Type 1 DM. But it does help us understand the mechanism.
My point was simply that hormonal status (specifically insulin status, although others are involved as well) may have much more to do with energy balance than how many calories go “in” and how many calories go “out.”
How do we account for amino acids and fatty acids that are used for structural aspects of metabolism (building/repairing tissue or enzymes) and are therefore not utilized as fuel? How do we address the down-regulation of metabolism that occurs when calories are restricted? The up-regulation of appetite that occurs when activity is increased? How do we explain the experimental results that show that, at the same calorie levels, low carb diets result in significantly (both statistically and clinically) more fat loss? The body is a complex system; the calories in-calories out concept is not without some significance, but it is only one piece of a very complicated puzzle.
Thanks for clearing that up, I understand your point better now. Also, as an aside, I think your embedded links might not be working. They aren’t for me anyway.
Glad that helped. Hmmm. I checked the links, but all seems well on this end. Of course that series of tubes and pipes is a complicated place–some e-rodents nibbling on the insulation somewhere, maybe?
By a strange coincidence, the person who set my wife and me on the track to health through low-carb eating was originally an engineer before becoming a (real) nutrition expert—Dr Barry Groves. His “Trick and Treat: how ‘healthy eating’ is making us ill” was a revelation, and his website at second-opinions dot co dot uk is a favourite starting point for all kinds of health enquiries.
He’s an excellent case-in-point. He was also one of my early resources for learning more about nutrition. I think there’s a lot of “nutrition-wise” engineers out there. They need to start a movement. I have a vision of nutrition lectures being given at IEEE conferences . . .
Hahah awesome, love that you used the classic RD illustration.
It’s the best. She looks exactly like my first grade teacher.
Love this, Adele! My husband, who is an engineer, would really appreciate it 😉 I love the cartoon too, lol!
It’s so easy to explain nutrition to engineers. If A then B then C. That’s it.