Mostly I just wanted to say “epic fail” because it embarrasses my kids, but then, they are always harshing on my mellow.
The stated goals of the US Dietary Guidelines are to promote health, reduce risk of chronic disease, and reduce the prevalence of overweight and obesity.

How’s that working for us?
First the good news. Cholesterol levels and hypertension have trended downwards since the creation of our first Dietary Guidelines.

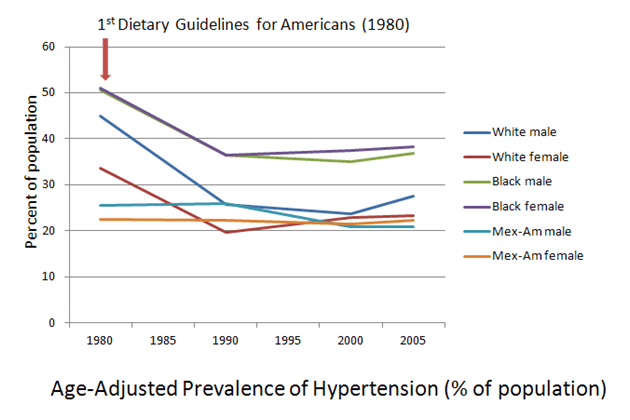
It is possible that the changes in these risk factors reflect a trend that was already well underway when the Dietary Guidelines were written . . .

. . . although some folks like to attribute the changes to improvements in our eating habits (Hu et al 2000; Fung et al 2008). And btw, yes, they actually have improved with regards to the dietary recommendations set for in our Guidelines. Don’t believe me? You’re not alone. Here’s the data.
Soooooo . . . if our diets really have improved, and if those improvements have led to related improvements in some disease risk factors (because cholesterol levels and even blood pressure levels are not diseases in and of themselves, but markers—or risk factors—for other disease outcomes, like heart disease and stroke), let’s see how the Guidelines fared with regards to actual disease.

This trend is a little ironic in that cancer was, at first, one of the primary targets for nutrition reform. It was Senator George McGovern’s ire at the Department of Health, Education, and Welfare’s (now the Department of Health and Human Services) failure to aggressively pursue nutritional links to cancer that was at least part of the motivation behind giving the “lead” in nutrition to the USDA in 1977 (Eskridge 1978; Blackburn, Interview with Mark Hegsted). In fact the relationship between dietary fat and cancer had so little solid evidence behind it, the 2000 Dietary Guidelines Advisory Committee had this to say: “Because relationships between fat intake and cancer are inconclusive and currently under investigation, they are deleted.”
I guess we can then feel assured that the reason that the restrictions against fat and saturated fat are still in the Dietary Guidelines is because their relationship to heart disease isn’t inconclusive or “currently under investigation”? If that’s the case, somebody better tell these folks. So what did happen to heart disease as we lowered our red meat consumption and our egg intake, while we increase our intake of “heart-healthy” grains and vegetable oils?

Well, you’d think with all of that reduction in fat and saturated fat, plus the decrease in smoking, we’d be doing better here, but at least—well, at least for white people—the overall trend is down; for black folks, the overall trend is up.
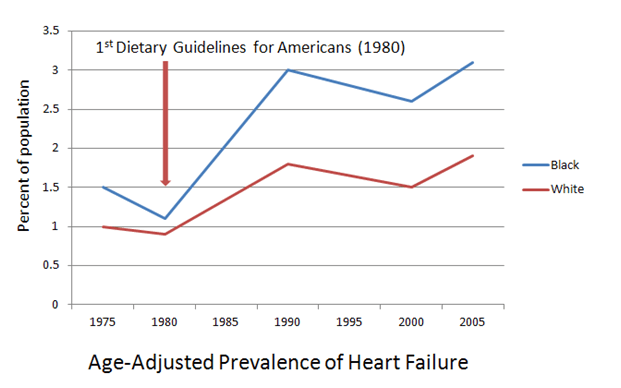
Oops. Not so good.

Hmmm.
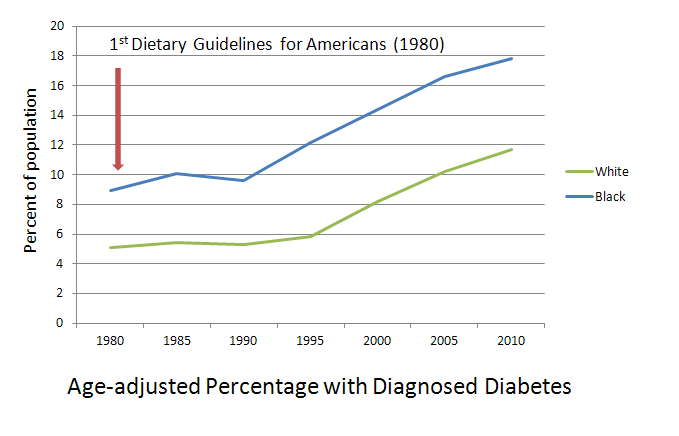
Oh. Well. This can’t be good. And of course, my favoritest graph of all:
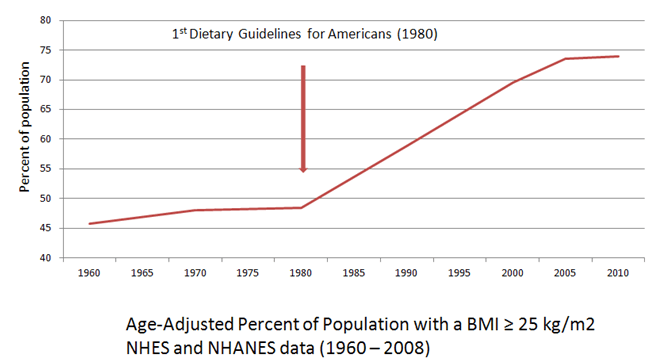
I’m not sure, but it sorta kinda looks like the Dietary Guidelines haven’t really prevented much, if any, disease. Maybe we could get those guys at Harvard to take a closer look? I mean, looking at these trends—and using the language allowed with associations—you might say that the development and implementation of Dietary Guidelines for Americans is associated with a population-wide increase in the development of cancer, heart failure, stroke, diabetes, and overweight/obesity. Anyway, you might say that. I would never say that. I’m an RD.
Are there other explanations for these trends? Maybe. Maybe not.
It’s always a good idea to blame food manufacturers, but we have to remember that they pretty much supply what we demand. And in the past 30 years, what we’ve demanded is more “heart-healthy” grains, less saturated fat, and more Poofas. Yes, food manufacturers do help shape demand through advertising, but the Dietary Guidelines don’t have anything to do with that.

Oh yeah. That‘s so whack, it’s dope.
References:
Blackburn H. Interview with Mark Hegsted. “Washington—Dietary Guidelines.” Accessed January 24, 2011. http://www.foodpolitics.com/wp-content/uploads/Hegsted.pdf
Centers for Disease Control and Prevention (CDC). National Center for Health Statistics, Division of Health Interview Statistics, data from the National Health Interview Survey. http://www.cdc.gov/diabetes/statistics/prev/national/figpersons.htm. Accessed 15 August 2010.
Centers for Disease Control and Prevention (CDC). National Center for Health Statistics, Division of National Health and Nutrition Examination Surveys. Prevalence of Overweight, Obesity, and Extreme Obesity Among Adults: United States, Trends 1976–1980 Through 2007–2008. http://www.cdc.gov/NCHS/data/hestat/obesity_adult_07_08/obesity_adult_07_08.pdf
Accessed February 1, 2011.
Eskridge NK. McGovern Chides NIH: Reordering Priorities: Emphasis on Nutrition. BioScience, Vol. 28, No. 8 (August 1978), pp. 489-491.
Fast Stats: An interactive tool for access to SEER cancer statistics. Surveillance Research Program, National Cancer Institute. http://seer.cancer.gov/faststats. Accessed on 11-1-2011.
Fung TT, Chiuve SE, McCullough ML, Rexrode KM, Logroscino G, Hu FB. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch Intern Med. 2008 Apr 14;168(7):713-20. Erratum in: Arch Intern Med. 2008 Jun 23;168(12):1276.
Hu FB, Stampfer MJ, Manson JE, Grodstein F, Colditz GA, Speizer FE, Willett WC. Trends in the incidence of coronary heart disease and changes in diet and lifestyle in women. N Engl J Med. 2000 Aug 24;343(8):530-7.
Morbidity and Mortality: 2009 Chart Book on Cardiovascular, Lung, and Blood Diseases. Bethesda, Md: National Institutes of Health: National Heart, Lung, and Blood Institute; 2009.
